Elevated Bone Mineral Density

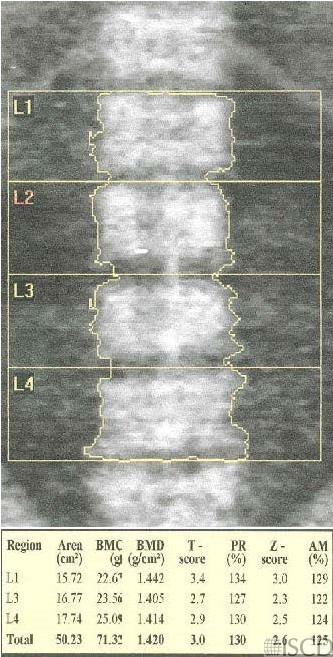
The Z-score is elevated in this Hologic lumbar spine DXA scan.
The Z-scores are also elevated at the femoral neck and total hip in the left proximal femur Hologic scan.
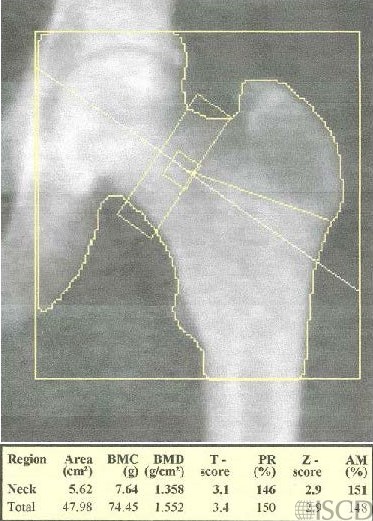
There is no International Society for Clinical Densitometry consensus on the definition of elevated bone mineral density. A paper by Dr. Michael Whyte (below in references) suggested that a Z-score >= 2.5 as a diagnostic criterion for elevated bone mineral density. Elevated bone mineral density has a wide differential diagnosis. No further work-up was available to evaluate a cause of elevated bone mineral density in this patient. There are elevated Z-scores at the lumbar spine and both sites in the left proximal femur.
Sarah L Morgan, MD, RD, CCD, The University of Alabama at Birmingham.
• Schwartz, J.B. and M. Rackson, Diffuse idiopathic skeletal hyperostosis causes artificially elevated lumbar bone mineral density measured by dual X-ray absorptiometry. J Clin Densitom, 2001. 4(4): p. 385-8.
• Blake, G.M. and I. Fogelman, Effect of bone strontium on BMD measurements. J Clin Densitom, 2007. 10(1): p. 34-8.
• Blake, G.M. and I. Fogelman, The correction of BMD measurements for bone strontium content. J Clin Densitom, 2007. 10(3): p. 259-65.
• Blake, G.M., et al., A review of strontium ranelate and its effect on DXA scans. J Clin Densitom, 2007. 10(2): p. 113-9.
• Kurland, E.S., et al., Recovery from skeletal fluorosis (an enigmatic, American case). J Bone Miner Res, 2007. 22(1): p. 163-70.
• Liao, J., et al., The effect of bone strontium on BMD is different for different manufacturers’ DXA Systems. Bone, 2010. 47(5): p. 882-7.
• Tamer, M.N., et al., Osteosclerosis due to endemic fluorosis. Sci Total Environ, 2007. 373(1): p. 43-8
• Whyte, M.P., Misinterpretation of osteodensitometry with high bone density: BMD Z > or = + 2.5 is not “normal”. J Clin Densitom, 2005. 8(1): p. 1-6.
• Bagur, A., V. Dobrovsky, and C. Mautalen, Bone densitometry of a patient with osteosclerosis. J Clin Densitom, 2003. 6(1): p. 67-71.
• Balseiro, J., D.F. Eggli, and H.A. Ziessman, Paget’s disease. A cause of artificially elevated bone mineral density. Clin Nucl Med, 1987. 12(10): p. 809-10.
• De Luna, G., et al., High bone mineral density in sickle cell disease: Prevalence and characteristics. Bone, 2018. 110: p. 199-203.
• Gregson, C.L., et al., Friend or foe: high bone mineral density on routine bone density scanning, a review of causes and management. Rheumatology (Oxford), 2013. 52(6): p. 968-85.
• Gregson, C.L., et al., ‘Sink or swim’: an evaluation of the clinical characteristics of individuals with high bone mass. Osteoporos Int, 2012. 23(2): p. 643-54.
• Hardcastle, S.A., et al., High bone mass is associated with an increased prevalence of joint replacement: a case-control study. Rheumatology (Oxford), 2013. 52(6): p. 1042-51.
• Balemans, W., et al., Increased bone density in sclerosteosis is due to the deficiency of a novel secreted protein (SOST). Hum Mol Genet, 2001. 10(5): p. 537-43.
• Bénichou, O.D., J.D. Laredo, and M.C. de Vernejoul, Type II autosomal dominant osteopetrosis (Albers-Schönberg disease): clinical and radiological manifestations in 42 patients. Bone, 2000. 26(1): p. 87-93.
• de Vernejoul, M.C., Sclerosing bone disorders. Best Pract Res Clin Rheumatol, 2008. 22(1): p. 71-83.
• Fosmoe, R.J., R.S. Holm, and R.C. Hildreth, Van Buchem’s disease (hyperostosis corticalis generalisata familiaris). A case report. Radiology, 1968. 90(4): p. 771-4.
• Fiore, C.E., et al., Hepatitis C-associated osteosclerosis (HCAO): report of a new case with involvement of the OPG/RANKL system. Osteoporos Int, 2005. 16(12): p. 2180-4.