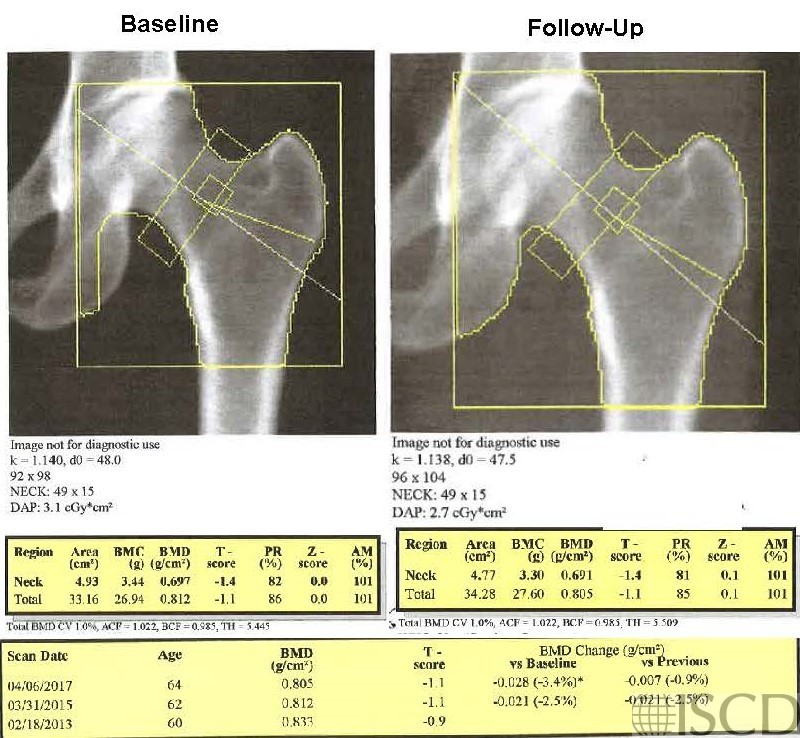
Wrong Hologic Total Hip Global Region of Interest Size on Follow-up

The upper left panel has the baseline scan. In the upper right panel the size of the hip global region of interest is not the same. On a Hologic scan, the size of the hip global region of interest, as well as the size of the femoral neck, in pixels is below the image. The bone map should be copied from the baseline to follow-up scan.
In this panel the global hip region of interest is now the same as baseline. The total hip bone mineral density is now less because less cortical bone from the femoral shaft is included in the total hip region of interest. Note that the sizes of the hip global region of interest, in pixels, are the same on the baseline and follow-up scan.
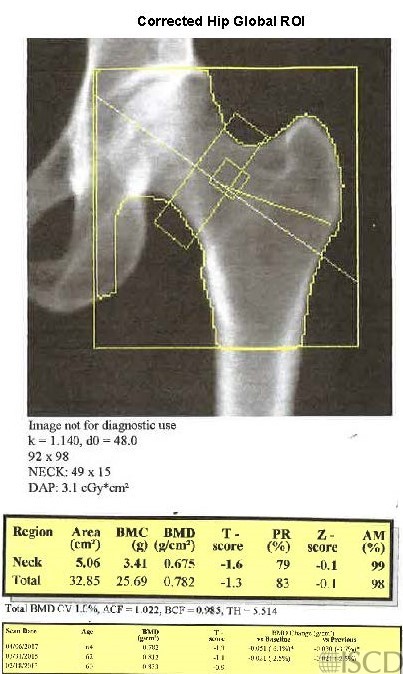
The size of the global hip region of interest is not the same in the baseline scan (upper left) and the follow-up scan (upper right). The bone map should be transferred and the size of the total hip global region of interest should be the same as on the follow-up and the baseline scan. The bottom panel shows the follow-up scan with the corrected global hip region of interest size. There is not a difference in the significance of change in this instance, using the institution 95% confidence intervals.
Sarah L Morgan, MD, RD, CCD, The University of Alabama at Birmingham