What is it?
Title: What Is It?
Submitted By: Lawrence G. Jankowski, CBDT Illinois Bone and Joint Institute, LLC Morton Grove, Illinois. USA
Patient History: A 71 yr old female, surgical menopause at age 43, with a diagnosis of osteoporosis and 13 year history of bisphosphonate exposure (9 years on oral alendronate or ibandronate, a three year drug “holiday” and one dose of zoledronic acid 5mg IV, one year ago). Past surgical medical history includes bilateral total knee replacements for osteoarthritis, and extensive multi-level lumbar spine fusion with hardware. She was referred to our osteoporosis clinic by her PCP as she was concerned about recent publicity of serious side effects of bisphosphonates, and has had chronic vague right thigh pain for many years.
Bilateral hip BMD and bilateral single energy femur scans were performed. Results of the bilateral hip DXAs as well as right femur frontal radiograph and corresponding coronal MRI are shown in figures 1 and 2 below, respectively. Left femur image (not shown) was unremarkable. 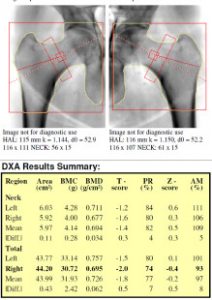 Figure 1: Bilateral hip DXA images and results
Figure 1: Bilateral hip DXA images and results  Figure 2: Single energy image of the right femur and coronal fluid STIR MRI of the right femur 8 years prior.
Figure 2: Single energy image of the right femur and coronal fluid STIR MRI of the right femur 8 years prior.
Question:
Is there imaging evidence for atypical femur fracture based on these images?
- AnswerThere is no evidence of focal lateral cortical thickening to suggest the development of an incomplete atypical femur fracture associated with long term bisphosphonate exposure.
- Discussion
Discussion: “Atypical” femoral fractures are fractures of the subtrochanteric/proximal femoral shaft which can occur spontaneously or with minimal trauma. A history of aching groin or thigh pain preceding the fracture is common as these are initially incomplete stress fractures which can go on to completely fracture with continued loading. On radiographs, a localized area of lateral cortical thickening with a beak-like appearance, with or without transversely oriented radiolucent fracture line can be seen1,2
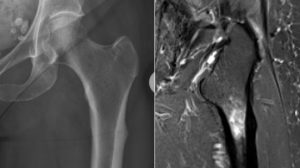 Frontal radiograph of the left hip (left image) and corresponding coronal STIR in another patient show beak-like lateral femoral cortical thickening (radiograph and MR), transverse fracture line (radiograph) and marrow edema (MRI). These findings are characteristic of atypical femoral fractures, incomplete in this case. The patient, upon a second interview of her medical history, revealed a distant history of osteomyelitis in her right femur. Serial radiographs and MRI showed stability of findings and were reported to be compatible with her history of osteomyelitis. The patient was told no further follow-up was required, thus did not think it important to mention. Based on her BMD, no history of new fractures, and normal PTH, vitamin D, and serum CTX in the pre-menopausal range, it was recommended that she not have another dose of bisphosphonate and to return in 2 years for a repeat DXA and reassessment at that time.
Frontal radiograph of the left hip (left image) and corresponding coronal STIR in another patient show beak-like lateral femoral cortical thickening (radiograph and MR), transverse fracture line (radiograph) and marrow edema (MRI). These findings are characteristic of atypical femoral fractures, incomplete in this case. The patient, upon a second interview of her medical history, revealed a distant history of osteomyelitis in her right femur. Serial radiographs and MRI showed stability of findings and were reported to be compatible with her history of osteomyelitis. The patient was told no further follow-up was required, thus did not think it important to mention. Based on her BMD, no history of new fractures, and normal PTH, vitamin D, and serum CTX in the pre-menopausal range, it was recommended that she not have another dose of bisphosphonate and to return in 2 years for a repeat DXA and reassessment at that time. Key Teaching Points: Often, patients may not be reliable historians, and unusual findings should be investigated more thoroughly before ordering an expensive battery of new tests. Atypical femoral fractures have characteristic imaging features and clinical characteristics. They occur after no/minimal trauma, and involve the lateral cortex of the proximal femoral shaft.
References:
- Chan, S. S., Rosenberg, Z. S., Chan, K. & Capeci, C. Subtrochanteric femoral fractures in patients receiving long-term alendronate therapy: imaging features. AJR Am. J. Roentgenol. 194, 1581–1586 (2010).
- Shane, E. et al. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 25, 2267–2294 (2010).